
Overview of the Texas State Tuberculosis (TB) Program, April 2008
April 24, 2008
The TB program conducts statewide activities to prevent and control tuberculosis among individuals who reside in Texas. The Department of State Health Services (DSHS) provides direct TB patient management through its Health Service Regions (HSRs) and supports the TB prevention and control programs of local health departments through contracts.
Written by Senator Eliot Shapleigh, www.shapleigh.org
The TB program conducts statewide activities to prevent and control tuberculosis among individuals who reside in Texas. The Department of State Health Services (DSHS) provides direct TB patient management through its Health Service Regions (HSRs) and supports the TB prevention and control programs of local health departments through contracts. The Texas Center for Infectious Disease in San Antonio and the University of Texas Health Center in Tyler provide hospital treatment of TB disease for those persons who cannot be managed in an out-patient setting. The program:
- Oversees three bi-national tuberculosis projects located on the Texas-Mexico border;
- Coordinates the Ten Against TB initiative which includes the six Mexican border states and the four U.S. border states;
- Monitors tuberculosis screening programs in county jails;
- Maintains a statewide registry of tuberculosis cases and their contacts; and
- Maintains a specialized registry of drug resistant tuberculosis cases reported to the State with a focus on multi-drug and extensive drug resistant cases.
The Texas TB Coalition and the Texas TB Epidemiologic Research Consortium are initiatives that seek to identify innovative approaches to the treatment and management of tuberculosis. The Heartland National Tuberculosis Center (HNTC, a CDC Regional Training Medical and Consultation Center) provides statewide tuberculosis expert consultant services at no cost to health care providers and local health departments. HNTC also develops and implements integrated and specialized curricula for professional training and education in all facets of tuberculosis elimination, treatment, case management, and testing strategies.
A) History
- The Texas Anti-Tuberculosis Association was organized in 1906. In 1912, the Registrar of Vital Statistics estimated that there were 43.208 cases of Tuberculosis in Texas. To deal with this serious and mounting problem, the Legislature created an Anti-Tuberculosis Commission in 1911 and authorized this Commission to establish a tuberculosis sanitarium. The Texas Sanitarium for the treatment of incipient pulmonary tuberculosis at Carlsbad, Texas opened on July 4. 1912. The Anti-Tuberculosis Commission was succeeded after the establishment of the Sanitarium by a Board of Commissioners for the Sanitarium.
- By 1925, the venereal disease program and tuberculosis control work had been delegated to the Bureau of Communicable Disease. The Bureau retained this title until the biennial reports of 1935 and 1936 when it was called the Communicable Disease Control and Epidemiology, and in the 1939-1940 reports, it is called the Division of Epidemiology.
- Before the advent of effective medical treatments for and control of active tuberculosis, the standard of care for TB was the sanitarium. By the 1940s and 1950s, Texas operated at least nine states-sponsored sanitariums.
- As medication and treatment progressed, and the disease became less prevalent in the United States, more and more attention was focused on prevention. The major responsibility for education was assumed by the State Tuberculosis Association and its local affiliates. The Tuberculosis Division had developed an educational program to complement those efforts. The Tuberculosis Division continued to supply lectures, small amounts of literature and statistical reports in an endeavor to acquaint the public with tuberculosis needs. The Division also acted as a clearing house for various agencies. The principal contributors to the clearing house of known tuberculosis cases are the Veterans Bureau, United States Public Health Service, other State Health Departments and local health departments of the United States, the Selective Service System, the State Sanatoria, cases found by positive sputum reports of the State Health Department laboratories, case-finding clinics conducted by the State Health Department and cases of tuberculosis provided by private physicians. A central registry of all known cases was maintained in the main office of the Tuberculosis Division.
- During the mid-1980s, the Tuberculosis Control Division focused more on community outreach, targeted tuberculosis testing in high risk populations and education and community awareness activities for the public at large. The Tuberculosis Control Division worked to strengthen the TB prevention and control activity in public health regions and local health departments.
- The state also began to close or transform its sanitariums during the 1980s. The one in San Antonio became the state’s hospital for severe cases of tuberculosis and other infectious disease. The South Texas Tuberculosis Hospital has evolved into an outpatient clinic. The East Texas sanitarium became the University of Texas at Tyler.
- In the 1990s, as tuberculosis cases continued to decline, the Tuberculosis Control Division was renamed the Tuberculosis Elimination Division. The Division worked to contain tuberculosis in urban areas and the border regions. These geographic areas of the state produced the majority of tuberculosis cases reported in Texas. The Division worked to build a strong TB training component for health professionals. A team of tuberculosis experts were established to consult on complicated tuberculosis cases. Contact investigation was strengthened to identify persons who may have been in contact with a person with tuberculosis. Early intervention to interrupt tuberculosis transmission was critical. In the 1990s, the Division created specialty units to work with high-risk areas where tuberculosis was still evident. The focus was on drug-resistant tuberculosis, tuberculosis in correctional facilities, tuberculosis and HIV infection, tuberculosis and diabetes, tuberculosis in the border region and tuberculosis in the foreign-born and minority populations.
- In 2000, the Tuberculosis Elimination Division was placed under the umbrella branch of Infectious Disease Intervention and Control. With the re-emergence of the disease, especially in its drug-resistant forms, the Tuberculosis Program now focuses on outbreaks, contact investigations and special TB incidents. The Tuberculosis Program continues to focus on high incidence areas in the state. Tuberculosis prevention and control activities continue to be applied to the elimination of tuberculosis in Texas. During the last three years, photofluorographic equipment has been available for mass case finding and county wide survey purposes. Since the use of the photofluorographic equipment for mass surveys has been placed into operation, approximately 750,000 have been x-rayed. There is a significant tuberculosis problem associated with the Texas-Mexico border, and the Tuberculosis Program has developed a bi-national effort to contain the disease in that region. However, it should be noted that the majority of tuberculosis cases in Texas are in its largest counties: Bexar, Dallas, Harris, Tarrant and Travis.
B) Funding
Funding for TB activities in Texas is derived from both state general revenue funds and federal Centers for Disease Control and Prevention (CDC) Cooperative Agreement funds. This combination of funds provides support for specific, essential components of TB prevention and control in the state (e.g., state laboratory services, TB program personnel, supplies, equipment, travel, and communication). Funds are provided to designated cities, counties and the state HSRs to support specific TB activities [e.g., directly observed therapy (DOT) for the treatment of TB patients and TB screening activities in jails and homeless shelters]. These funds also support extensive reporting and surveillance activities, expert TB consultative services and contact investigation.
| Appropriations | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
| Expended | Expended | Expended | Expended | Estimated | Budgeted | |
| General Revenue | $12,664,977 | $11,368,811 | $12,928,621 | $11,609,736 | $12,497,974 | $14,902,326 |
| Federal Funds | $5,055,886 | $6,092,011 | $5,613,347 | $6,860,434 | $7,443,876 | $7,306,052 |
| Other Funds | $58,462 | $476 | $53,412 | $0 | $12,561 | $0
|
| Total All Funds | $17,779,325 | $17,461,298 | $18,595,380 | $18,470,170 | $19,954,411 | $22,259,388 |
In addition to these amounts, the state spends approximately $20 million per biennium on the Texas Center for Infectious Disease, which treats difficult cases of tuberculosis and other infectious diseases. The 80th Legislature appropriated $32 million in General Obligation bond funds (HB 1) for the construction of a new tuberculosis hospital.
C) FTEs
Currently, the DSHS TB program has a total of 112 FTEs; 73 are assigned in the HSRs and 39 at the DSHS central office in Austin. Local health departments fund additional FTEs for TB Prevention and Control. Herein below is a chart detailing the number of FTEs per year for the last five years.
| FTEs | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
| Actual | Actual | Actual | Actual | Estimated | Budgeted | |
| 133.3 | 125.0 | 110.1 | 111.7 | 111.5 | 128.6 |
D) Experts
The state TB program has a staff with expertise in epidemiology, contact investigation, evaluation, and outbreak management. The DSHS Laboratory also has expertise in TB studies such as cultures, sensitivities, and other methods of identifying specific TB organisms to support clinical care as well as surveillance. The state TB program provides support and technical assistance to regional and local health department TB programs in Texas. Medical expertise is available to DSHS and consultations are available to Texas physicians treating complicated cases from the following expert physicians: Dr. Barbara Seaworth at the Heartland National TB Center in San Antonio; Dr. David Griffith and Dr. Peter Barnes at the University of Texas Health Center at Tyler; Dr. Kim C. Smith at the University of Texas Medical School at Houston; Dr. Manuel Rivera at Texas Tech University Health Sciences Center in El Paso; and Dr. Jeffery Starke at the Baylor College of Medicine in Houston.
E) Cost of infectious TB patient to the public health system
DSHS purchases medications at very low public sector prices for the treatment of TB and latent TB infection and distributes these medications without cost to local health departments in Texas that provide TB services. Based on drug prices in the fall of 2006, the cost of medication to treat a person for 9 months with the standard recommended therapy for disease that is sensitive to the first-line medications is about $310. The cost rises to about $25,000 for two years of medication for a person whose TB organism is resistant to the two most effective drugs, which are isoniazid and rifampin.
The drug costs for persons with more extensive drug resistant TB rises significantly depending on the resistance pattern. Since the second-line medications are also known to have significantly more adverse drug reactions, the patients are frequently hospitalized for long periods of time at the Texas Center for Infectious Disease so that their treatment progress may be monitored more closely than is possible in an out-patient setting. Hospitalization adds significantly to the cost of care for these patients. In a study that was conducted by the CDC and published in 2004 on the costs of patients hospitalized for multi-drug resistant TB, it was estimated that the average total costs per person for those who survived was $89,594, and the average cost of hospitalization for those who died was $717,555. The total costs for patients with multi-drug resistant TB in the study ranged from $28,217 to $1,278,066. Medication costs to treat someone for latent TB infection in order to prevent more expensive TB disease are about $8.
The cost of medication is only a small part of the cost of treatment and the public health response of contact investigation, which includes the medical evaluation of contacts and their treatment if infected. Diagnostic tests for the medical evaluation of a person suspected of having TB disease include a tuberculin skin test ($10), a chest radiograph ($25-$100 per view depending on the contractor and whether interpretation is included), and three sputum smears and cultures ($360). Since many more persons are evaluated for suspected TB disease than are confirmed as having TB disease, the costs to public health are greater than the cost of evaluation times the number of cases for any one year. Depending on the location of the patient, a hospital district may bear the cost of evaluation. In rural areas, the DSHS regions provide and/or pay for the medical evaluation.
Three DSHS laboratories (in Austin, San Antonio and Harlingen) and three major metropolitan health department laboratories (Dallas, El Paso and Houston) perform sputum smears and cultures. Other laboratory tests that are required to monitor for adverse drug reactions and response to therapy include those for liver and kidney function, complete blood counts, as well as frequent follow-up AFB smears and cultures. Patients on certain anti-TB medications must also be monitored for changes in visual acuity, color discrimination, and hearing.
The labor costs for public health workers contribute significantly to the cost of providing services for the treatment of TB. The standard of care in Texas is to provide directly observed therapy (DOT) for each person with TB disease. A trained health care worker asks the patient about symptoms of adverse drug reactions before each dose of medication and then observes the patient taking the medication. Additionally each patient receives a monthly nursing assessment for adverse drug reactions and clinical response to therapy.
One of the most variable costs associated with the public health response to an occurrence of TB disease is the contact investigation and subsequent screening and treatment of the contacts for latent TB infection. If a congregate setting is involved (such as a worksite, school or nursing home), there may be several hundred persons who must be located, tested for TB infection, and screened for symptoms of TB disease.
F) Statistics
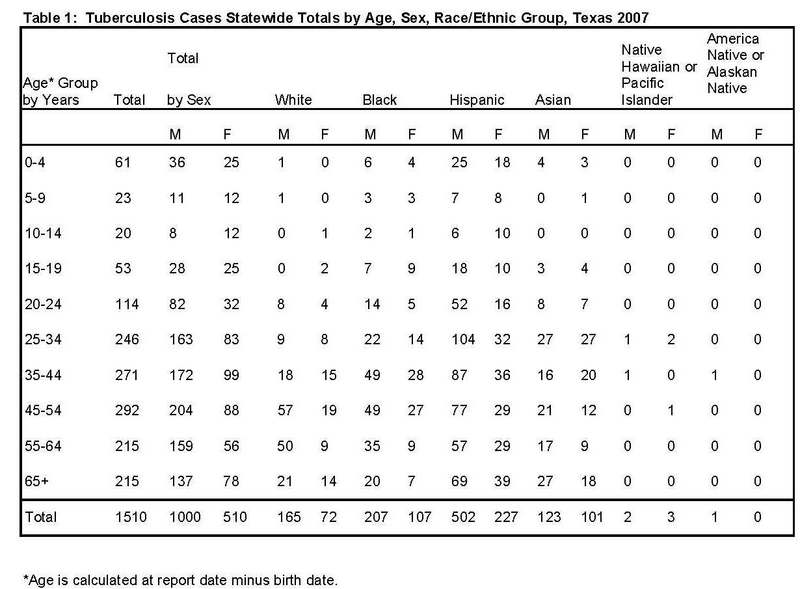
The state of Texas reported 1,510 TB cases in 2007 for a case rate of 6.3 cases per 100,000 population. This is a 4.7% decrease from the 1,585 cases reported in 2006. In 2006, Texas ranked second in the number of cases behind California (2,779 cases) and ranked fourth in rate behind Alaska (10.4), Hawaii (8.9), and California (7.6).
TB in Texas is disproportionately represented in racial and ethnic minorities (Table 1). In 2007, Whites represented 15.7% of the reported TB cases, Blacks represented 20.8%, Hispanics represented 48.3%, and Asians and others represented 15.2%. Hispanic children nine years of age or younger accounted for 69% of the cases in the 0-9 age group. Most of the TB cases reported in 2007 were in males (66%).
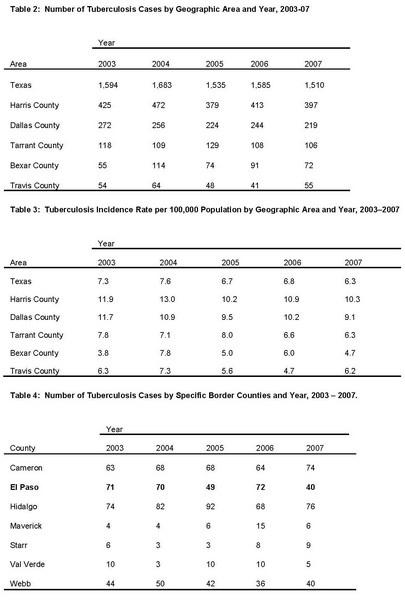
For 2007, the large urban areas of the state and several counties along the Texas-Mexico border reported the greatest percentage of TB cases. The majority of TB cases reported in Texas come from the five major population areas of the State. These counties and their corresponding largest cities are Harris County (Houston), Dallas County (Dallas), Tarrant County (Fort Worth), Bexar County (San Antonio), and Travis County (Austin). They represent 56.2% of the State’s TB morbidity. One of these five major metropolitan areas reported an increase in TB morbidity in 2007 (Table 2). The incidence rates per 100,000 population for the State and the five major population areas by year are shown in Table 3.
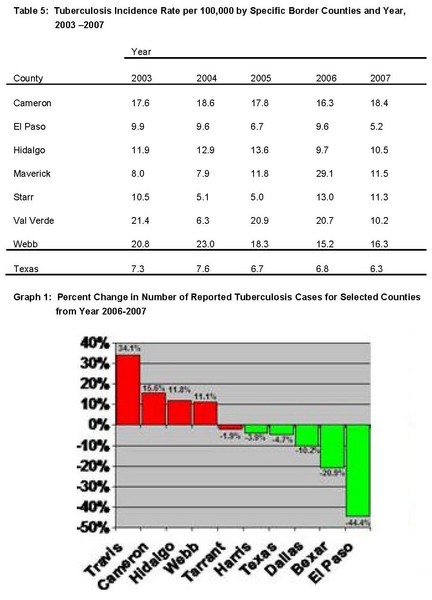
The number of cases reported in the major border counties of Cameron, El Paso, Hidalgo, Maverick, Starr, Val Verde, and Webb are detailed in Table 4. Four of these border counties experienced increases in morbidity for 2007. The incidence rates for these counties are detailed in Table 5.
Graph 1 depicts the percentage change in the number of reported TB cases for the major counties in Texas, four of which (Cameron, El Paso, Hidalgo and Webb) are located along the Texas/Mexico border.
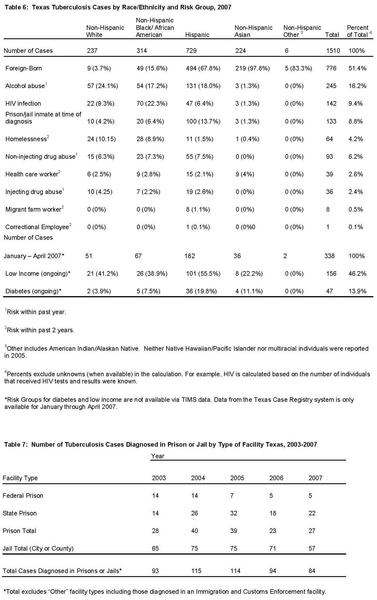
In Texas, foreign-born persons continue to account for a significant percentage of the TB morbidity. The percentage of foreign-born TB cases has steadily increased over the past 5 years from 45% in 2003 to 51% of cases reported in 2007. Foreign-born persons represented 47.9% (760) of the TB cases diagnosed in Texas in 2006. In 2007, foreign-born persons represented 51.4% (776) of the TB cases diagnosed in Texas.
In 2007, there were 61 different countries represented among the foreign-born persons with TB reported in Texas. Of the 776 foreign-born TB cases, 49.2% reported Mexico as the country of origin, 8.6% reported Vietnam, 6.2% reported Honduras, 5.5% reported India, 5.2 % reported Philippines, 3.1% reported El Salvador, 2.8% reported Guatemala, and 2.1% reported China. In 2007, 42.4% percent of the TB among foreign-born persons was reported within five years of arrival to the U.S. while 45.5% had resided in the U.S. ten or more years from their arrival date to the date TB was reported.
Specific risk factors such as low income, alcohol, substance abuse, incarceration, and HIV infection contributed to TB morbidity. In 2007, persons who abused alcohol accounted for 16.2% of cases, persons with non-injecting drug abuse accounted for 6.2% of the cases; persons with HIV/AIDS accounted for 9.4%; and persons who were incarcerated, in a jail, prison or other correctional facility, at the time of diagnosis accounted for 8.8% of cases. Many persons with TB have multiple reported risk factors. See Tables 6 and 7.
Click here to view larger image.
Click here to view larger image.
Click here to view larger image.
Click here to view larger image.
For further information related to TB prevention and control activities in Texas, contact Charles E. Wallace, Ph.D., M.P.H., Manager of the DSHS Infectious Disease Intervention and Control Branch at 512-458-7111 ext 2291 or via email at charles.wallace@dshs.state.tx.us.